Full-Featured Electronic Prescribing

OnCallData is the FIRST two-way electronic prescribing service between physicians and pharmacies.
OnCallData provides a rich, full-featured electronic prescribing system with state-of-the-art medication reconciliation, electronic prescribing of controlled substances (EPCS), drug utilization review, real-time formulary and patient benefits checks, electronic prior authorization services, and prescription drug monitoring program (PDMP).
OnCallData provides a rich, full-featured electronic prescribing system with state-of-the-art medication reconciliation, electronic prescribing of controlled substances (EPCS), drug utilization review, real-time formulary and patient benefits checks, electronic prior authorization services, and prescription drug monitoring program (PDMP).
Electronic Prescribing Controlled Substances

OnCallData?s certified EPCS solution provides state-of-the-art security for any Internet-connected devices.
Both USB security tokens and Mobile Authentication are supported. For more details on OnCallData EPCS,
click here.
Electronic Prior Authorization
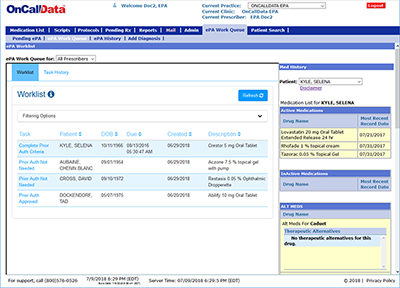
OnCallData checks if a drug requires prior authorization (ePA) within seconds, and within the script-writing workflow.
Most ePA decisions are completed within an hour, and all ePAs are tracked by OnCallData support. For more details on
OnCalLData?s ePA solution, please click here.
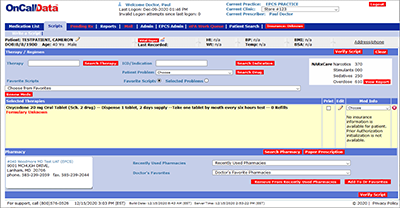
Real-time Formulary and Benefits Check
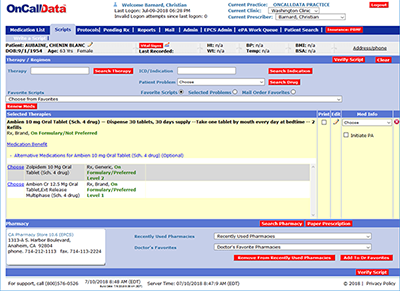
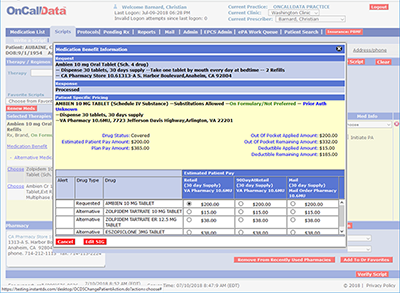
OnCallData provides patient formulary status of a drug, drug alternative formulary statuses, and coverage-level
specifics for a drug in real-time and within the script-writing workflow; an additional click provides
real-time patient benefits, including copay, deductible information, and relative costs of mail order
and longer-term prescriptions.
Prescription Drug Monitoring Program
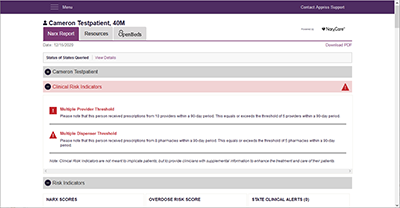
Many states require providers to participate in a Prescription Drug Monitoring Program, tracking patient
narcotic prescriptions. OnCallData is integrated with a third party, Bamboo Health, which provides the gateway
for many states programs. Through this integration, you are able to fulfill the state PDMP requirements.